
by Dr. rer. physiol. Michael Ue bele, formerly head of the Physiotherapy School
at Johannes Gutenberg University Mainz
Video Analysis – evidence-based work within the clinical reasoning process
In addition to the medical history, observing the patient’s motor behavior is an essential part of the clinical reasoning process (CR process) in physiotherapy.
The musculoskeletal system’s problems reveal themselves to the trained therapist’s eye in the form of compensation mechanisms, for example disturbed link chain reactions, changed myofascial reactions, etc..
The observation of motor function processes in the CR process leads to initial hypotheses regarding the possible causes of the malfunction. The formation of hypotheses influences the selection of suitable test procedures in order to review and prove the evidence of therapeutic interventions.
The analysis of motion can be facilitated and optimized by video recordings.
The main advantages of video analysis are:
- Improvement of the therapist’s optical diagnostic skills
- Objectification of the findings
- Documentation of findings and progress made
- Traceability of findings and therapy results by therapist and patient
- Evidence of therapeutic interventions
Video Analysis in Physiotherapy Practice
In addition to my “normal” physiotherapeutic activity based on medical prescription, I offer movement analysis as an additional physiotherapeutic service, a second health market.
Movement analysis is mainly used by amateur and competitive athletes who have problems during their sport or who want to optimize their training. The following case description shows how video analysis is integrated into the physiotherapeutic process by recording findings and the subsequent therapeutic interventions.
1. Case Description
It is the 64-year-old amateur runner “AT”, who trains an average of 3 times a week and has a training scope of 40 to 50 km per week. He is currently preparing for a half marathon that will take place at the end of May (age group 65 – 70 years).
Aside from pain in his right knee, which increases as he runs, Mr. “AT” has no physical problems. However, he has the feeling that his run “no longer feels so smooth” and that he “is currently running below his potential”. From the movement analysis, he promises to get information about whether technical deficits can be defined and whether they can be minimized or remedied through targeted training measures.
The running analysis was performed on a treadmill and with a video camera and the iPad set EIDOO and evaluated with the video analysis program Dartfish 9.0 Pro Suite.
Results of the Visual Examination
The decisive compensation mechanisms of “AT” can be seen, both in “barefoot running” and in running with his sports shoes in the shock absorber phase.
Note: The shock absorber phase represents a decisive phase within the individual stance phases. In this phase, high torque forces occur (flexion torques of the trunk and hips, adduction torque of the pelvis, adduction and internal rotation torque of the thigh, eversion torque on the rear foot, etc.) which respond muscularly. In this phase, in particular, the corresponding skeletal muscles (global stabilizers) are stressed in their concentric and eccentric mode of operation, depending on the direction.
The shock absorber phase of the left lower extremity (viewed from the dorsal side) shows the following abnormalities (videos 1 and 2, key positions 1/1 and 2/1 ):
- the strongly laterally directed foot
- a visible eversion torque of the rear foot (global pronation)
- the adducted position of the lower extremity
- a visible torque of the pelvis (sinking to the right)
- lateralization of the trunk to the left
- a clearly visible abduction of the left upper arm in the swing phase (shoulder flexion).
The laterally aligned foot and the adducted position of the lower extremity can also be demonstrated in the shock absorber phase of the right lower extremity (videos 1 and 2, key positions 1/2 and 2/2 ).
In this phase as well, the left arm is held in clearly visible abduction in the extension phase of the shoulder joint. In contrast to walking barefoot, however, the adduction of the lower extremities is reduced (see ibid.).
The adducted alignment of the right and left lower extremities is maintained until the rolling phase ( video 1 and 2, key positions 1/3, 1/4 or 2/3 and 2/4 ). In contrast to barefoot running, the adduction of the respective lower extremity is reduced when running with sports shoes.
In the side view, the relatively low hip extension in the final standing phase or the pushing-off phase is noticeable on both sides, which is compensated for on the right and left with “excessive” knee flexion ( cf. video 3, key position 3/1 and video 4 key position 4/1.
The different stride lengths are also noticeable in the side comparison ( video 3, key position 3/2 and video 4, key position 4/2 ).
3. Further Findings and Test Results
The visual examination of both feet in the supine position shows deficits in the distal arches of the foot. The “subluxated” position in the area of the metatarsophalangeal joints indicates that the local stabilizers (Mm. Lumbricales and interossei) no longer optimally stabilize the metacarpal joints and the global stabilizers (toe flexors and toe extensors) influence this link chain in the sense of a compensation mechanism (“gooseneck deformity”, see pictures 1 and 2 ).


With the exception of the movements of the Chopardian joint line, all the joints of the lower extremities are freely movable and do not show any differences from each other. Mr. “AT” has deficits on both sides with regard to the “selective” movement in pronation (common line of Chopart).
The strength tests of the skeletal muscles in the lower extremities did not show any positive results in a side comparison (all strength values of the leg muscles tested were in the range of full strength: 5/5).
Note: Because defined strength tests test "open chain" muscles, these strength tests do not correspond to "closed muscle chain" functional conditions.
The length tests concerning the ventral and dorsal myofascial chain show clear deficits in elasticity in the hamstrings and in M. iliopsoas and M. rectus femoris (see photos 3, 4, 5 and 6) as well as in the area adductors.




The rotation test of both hips reveals a significant restriction in internal rotation ( see Figure 7 and Figure 8 ).


Movement control tests provide further information on whether there are deficits in the motor control system.
The following tests show positive results:
- “Prone Lying Knee Flexion” – on the right; a deflection of the pelvis in the sense of rotation can be determined ( see: Video 5 ).
- “One Leg Stand” – when performing the one-leg stand on the left, a clear deflection of the navel in the frontal plane with pelvic rotation is visible ( Video 6 ).
- “Sitting Knee Extension” – when the left and right lower leg are extended, a kyphotic deflection of the lumbar spine can be detected.
4. Interpretation of the Findings
Running speed is the product of stride length and step frequency. Both parameters depend on the elasticity of the ventral and dorsal myofascial chain. The corresponding findings from Mr. “AT” explain the deficits with regard to hip extension, which in turn affect the stride length.
The short step length on the right compared to the sides (left leg push-off phase – right leg initial) speaks for a temporally reduced stance phase of the left lower extremity, as well as for the plane foot contact in the initial contact phase of the right foot. The lower stretchability of the hamstrings of the right lower extremity compared to the sides, could also serve as an explanation for the flat footrest in addition to the side difference.
Note: With the beginning of the final standing phase up to the roll-off or push-off phase, the abductor and internal rotatory muscle activity should increase, which should also be documented in the corresponding joint position of the hip as well as in the plantar flexor and pronator muscle activity of the "standing foot. This muscle synergy leads to optimal power transmission from “the big toe to the center of gravity (KSP)”.
The end stance and push-off phases of Mr. “AT” are characterized by a predominantly adductive and externally rotatory joint position of the stance phases. The reasons for this could be the lack of internal rotation of both hip joints, as well as the high tone of movement or lack of eccentric activity of the adductors. The high number of repetitions of the step cycles certainly also contribute to the fact that this compensatory movement pattern is called up automatically.
This prevents the phase of switching into the extensor, abductor, and internal rotational movement patterns that are so important for a runner.
Another weak point in Mr. “AT” is the inadequate erection of the feet. The strong lateral load on the calcaneus in the initial contact phase, causes a large eversion torque within the immediately following shock absorber phase, which the muscular system responds to inadequately (pes valgus, global pronation or “buckled foot position”). This foot position is maintained until the rolling phase and leads to increased stress on the distal transverse arch (“penetrated” transverse arch – see visual findings on the feet).
The coordination problems in both closed muscle chains are particularly evident in the left shock absorber phase, during which the adduction torque is answered inappropriately by the muscles (sinking of the pelvis). The deflections of the trunk and the clearly abductive posture of the left swing arm can be understood as compensation mechanisms to compensate for the “deficiency” in the closed muscular chain.
Goals and Measures
The exercise program developed for Mr. “AT” aims to work through his deficits, with the goal of optimizing his running technique and taking away the feeling of “heaviness” when running.
A large number of findings require an extensive “exercise program”, but this must be tailored to the conditions of a “hobby runner” and his daily training routine. The aim of the training plan is to cover the range of findings with relatively few exercises.
Since the quality of the exercise is the decisive criterion for optimizing the stance and swing phase pattern, the exercises must be carried out with full concentration and in a non-exhausted state.
Furthermore, the exercises are carried out without exception in the “closed muscle chain” in order to keep the transfer loss to the target exercise (stance phases while running) as low as possible.
5. Training Plan
Exercise: “Bridging”
By means of the exercises in bridging, the co-activation processes of muscle synergies in the stance phase are trained under changed gravity conditions. The decrease in torso weight allows special consideration of the upright position of the feet, in order to create optimal conditions for transferring impression forces to the KSP.
Furthermore, the exercises are ideally suited for working through the motor deficits of segmental instability in the LBH region.
Important parameters for the execution of the exercise are:
- Foot load: In the case of “AT” the two calcaneal tuberosities medial and lateral should be in contact with the surface, as should the metatarsophalangeal joint of the big toe.
- The knees are aligned axially.
Exercise implementation:
- Eyes seek contact with the knees (beginning of activation of the ventral muscle chain).
- A conscious strain is sought on the lateral calcaneal tuberosity and the metatarsophalangeal joint of the big toe, with the knees oriented anteriorly towards the feet.
- The muscle synergies within the co-activation process are activated by the load on the feet.
Visible signs of this activation are:
- Retraction of the navel in a dorsal direction (activation of the local stabilizers of the LBH area (M. transversus abdominis, diaphragms thoracic, and pelvis).
- “Tension” of the dorsal myofascial muscle chain from the point fixed (pf) Calcaneus (M. triceps surae, ischiocrual muscle group, M. adductor magnus, M. gluteus maximus, abductors).
- Alignment of the spine in the “neutral position” with the tension of the ventral myofascial muscle chain in its effective direction cranially.
- Raising the pelvis until the hips are extended. (See picture 9 ).
Exercise 1a: “static” holding in bridging
Taking the above parameters into account, the pelvis is moved into extension and held in this position. The holding period depends on the ability of the trainee to carry out bridging correctly and without evasive mechanisms. ( See picture 9 ).
In the case of Mr. “AT”, a holding period of 20 seconds was defined.
Load normative:
3 Serien at 20 sec, ½ Minute Pause
Increase: Increase the holding time by 5 seconds or increase the series by 1 series

Exercise 1b: “dynamic” bridging
The pelvis is moved up and down in a controlled manner without leaving the neutral zone (NZ) of the spine (WS). The number of repetitions depends on the ability of the practitioner to perform the exercise correctly. (See video 7 and key position 7/1 ).
Load normative:
3 series of 12 repetitions, half a minute break
Increase: Increase the repetitions by 2 repetitions or increase the series by 1 series.
Exercise 1c: “static” one-legged bridging
From the position of exercise 1a (“static bridging”) one leg is moved into the step phase until a hip and knee flexion of 90 ° each is achieved (open chain). The NZ of the WS and the axially aligned position of the lower extremity must not change (note: no sinking of the pelvis on the free leg side). ( See video 8 and key position 8/1 ).
Load normative:
Holding time: 10 sec, series: 3, pause: takes place by changing legs.
Increase: Increase the holding time by 2 seconds or increase the number by 1 series.
Exercise 1d: “Dynamic” one-legged bridging
The starting point is exercise 1c . From this position the pelvis is continuously brought back to the base and back to the starting position. The WS of the WS remains unchanged.
Load normative:
Number of repetitions: 8, series: 3, break: takes place by changing legs
Increase: increase the number of repetitions by 1 repetition or increase by 1 series.
Evasion mechanisms:
Since the quality of the exercise is decisive for the training effect, the exercises must be carried out under guidance and control (perception training) .
Mr. “AT” must be made aware of the following compensation mechanisms by means of kinesthetic stimuli:
- Loss of eversion control (foot “drifts” into a global pronation (buckle foot position) (See Figure 10 ).
- The big toe cannot hold the abduction and moves laterally. (See image 10.)
- The respective knee of the supporting leg deviates in adduction. ( Fig. 10 )
- The WS of the WS is lost during the exercise and an increased lordosis arises, or the pelvis tilts to the “free leg side”.

Exercise 2: side plank
The side plank is an asymmetrical starting position in which the lower extremities (support arm and support leg) each build up a punctum fixum. The upper extremities lie close to the body. The spine is stabilized in the NZ. Side plank exercises place high demands on the global and local stabilizers of the pelvic-trunk region and particularly integrate the hip abductors to work in the closed muscle chain.
Exercise 2a: “Static” side plank with knee flexion
Bilateral knee flexion (90°) increases the body’s support surface and facilitates trunk stabilization. After picking up the support, the pelvis is raised, the spine is aligned in the NZ and then stabilized (image 11).
Load normative:
Holding time: 15 sec, pause: by changing sides, series: 3
Increase: Increase holding time by 3 seconds or increase the number of series by one series

Exercise 2b: “dynamic” side support with knee flexion
After taking the side support, (see exercise 2a) the pelvis is continuously moved to the base and back to the starting position (ASTE). ( Video 9 ).
Load normative:
Number of repetitions: 8, pause: takes place by changing sides, series: 3
Increase: Increase the number of repetitions by 2 repetitions or increase the number by 1 series.
Exercise 2c and Exercise 2d:
“Static” and “dynamic” side support with extended legs ( Video 10 ).
After about 2 weeks, exercises 2a and 2b are replaced by exercises 2c and 2d.
The load norms remain the same. Leg extension places, increased demands on postural control and balance. Within the closed muscle chain, the demands on the hip abductors are increased.
Evasion mechanisms:
In the position of the side support, the stabilization of the NZ cannot be maintained and the practitioners avoid hyperlordosis or lumbar spine kyphosis. Furthermore, the pelvis cannot be held in the frontal plane and it describes a rotation in an anterior or posterior direction.
In the case of Mr. “AT”, the exercise results in subtle deflections into the lumbar spine kyphosis, with accompanying convex deflection of the lumbar spine to the upper side ( Figs. 12 and 13 ).


Exercise 3: Movement transition from sitting to standing
This seemingly simple task gets its degree of difficulty from the special consideration of the upright position of the feet and the correct axis positioning of the thigh, when performing the exercise. When performed exactly, the practitioner feels the high load on the muscles that lift the feet and their training effect.
The exact positioning of the calcaneus in the initial sitting position is decisive. In the case of Mr. “AT”, the two calcaneal tuberosities, as well as the metatarsal heads I and V, should be consciously felt. Thereafter, the exerciser should consciously load the lateral calcaneal tuberosity and the metatarsophalangeal joints (spiral statodynamic twisting of the foot through inversion of the rearfoot and pronation of the forefoot).
The load on the foot must not change while standing up. The knees are aligned axially and should not change this position while standing up and sitting down. The WS is stabilized in the NZ ( video 11, key position 11/1 ).
Getting up and sitting down is carried out so slowly that the practitioner can stop the movement at any time.
Load normative:
Repetitions: 10 repetitions, series 3, rest ½ minute
Increase: Increase the number of repetitions by 2 repetitions or increase the series by 1 serie
Evasion mechanisms:
- The feet lose the stress points and give way to a “buckle foot position” (Pes Varus).
- One or both knees give way in adduction or abduction.
- The toes “claw” during the exercise.
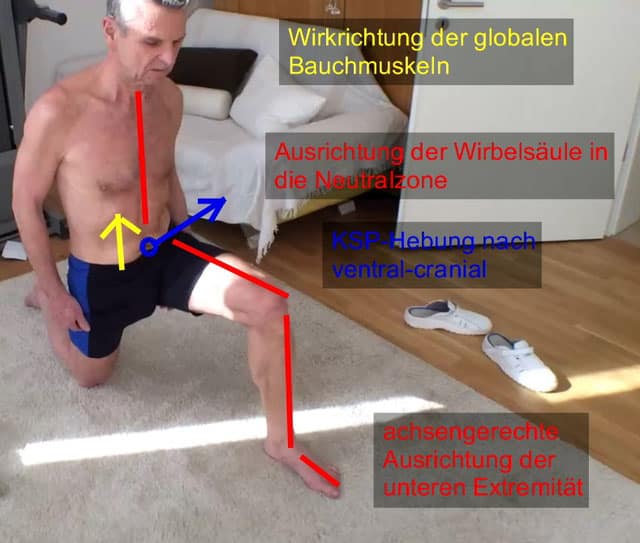
Exercise 4: Einbeinkniestand Appears to be in another language? Not sure?
The one-legged kneeling position is a very complex and functional exercise, as it trains muscle synergies in the closed muscle chain in an abstract form, which occur in the double stress phase of walking. The “final stance phase” of the rear leg requires hip extension, while the “shock absorber phase” of the front leg increasingly takes on the body weight.
Exercise 4a: “static” one-legged kneeling position
The knee flexion of the front leg is 90 ° and the foot adjustment is carried out in the same way as in exercise 3 (sitting position). The lower leg of the rear leg rests axially on the floor, the rear foot finds its pf on the distal transverse arch. The upper body stays upright in the room (NZ of WS).
The practitioner imagines lifting his/her KSP forward and upward so that more and more weight is shifted to the front leg. The tensing of the sciocrural muscle group and the adductor magnus muscle should be clearly noticeable.
At the same time, the practitioner activates his abdominal muscles with the intention of pulling his pelvis towards the cranial side. With the accompanying “pelvic adjustment”, the rectus femoris muscle has to relax eccentrically (feeling of stretching in the ventral area of the thigh) ( Fig. 14 ).
Load normative:
Holding time 15 sec, series: 3, pause takes place by changing the standing leg
Increase: the holding period is increased by 5 seconds or the number of series is increased by one series.
Exercise 4b: “dynamic” one-legged kneeling position ( see video 12 )
Building on exercise 4a, the practitioner raises and lowers his KSP forwards and upwards (approx. 15 to 20 cm)
Load normative:
Number of repetitions: 5, series: 3, break is made by changing the standing legs.
Increase: Increase the KSP elevation by approx. 5cm each time, increase the number of repetitions by 2 repetitions, or increase the series by 1 series.
Objective: to get up from the one-legged kneeling position without any evasive mechanisms.
Evasion mechanisms:
- Loss of the upright position of the foot (in the case of AT: pes valgus).
- Adduction-internal rotation tendency of the front leg.
- Excessive knee flexion (as a result, the quadriceps muscle takes on the main task of verticalization and the dorsal muscle chain “loses” its anti-gravitational effect).
- The WS of the WS is lost and the practitioner deviates into a “hyperlordosis” or a kyphotic posture.
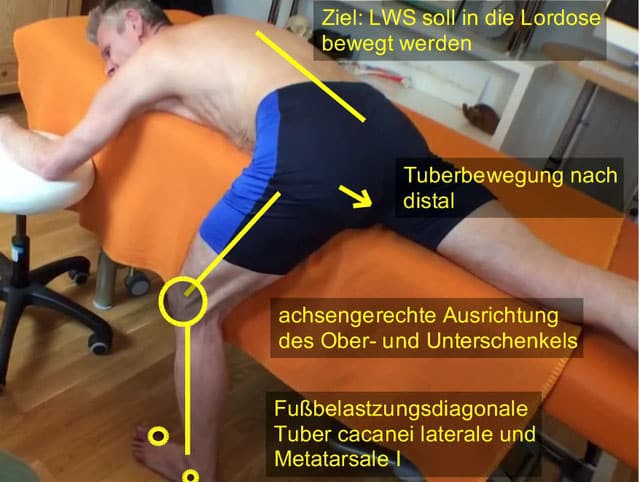
Exercise 5: Lie on your stomach with your leg down
In the case of Mr. “AT”, the focus of this exercise is on the eccentric relaxation of the dorsal myofascial chain. The functionality of this exercise is based on the fact that the stretching takes place in the closed muscle chain.
From the prone position on the treatment bench, one leg is placed on the floor. The sciatic tuberosity and the calcaneus should be in line. The feet are adjusted according to the aspects described in exercise 3. The knee is slightly bent. The practitioner tries to move his pelvis from the “kyphotic” position towards the “lordosis” by aligning the ischial tuberosity “caudal-dorsally”. Initially, the therapist has to facilitate the pelvic adjustment with the help of kinesthetic stimulation, in order to give the practitioner the appropriate sense of perception for his pelvis. If the “pelvic adjustment” is successful, there is an enormous stretch in the parts of the myofascial chain in which “shortenings” have manifested. (See picture 15.)
Load normative:
“Stretching time”: 10 sec, 2 series, break is made by changing legs
Increase: “The duration of the stretch is increased by 3 seconds each time
Evasion mechanisms:
- During the exercise, the knee is extended without the pelvis moving into the lumbar spine.
- The knee of the “supporting leg” gives way in adduction and internal rotation.
- The foot of the standing leg loses its upright position. (See exercise 3 and 4.)
Exercise 6: standing abductor training ( see video 13 )
To stabilize the stance, the practitioner supports himself with both hands on a door frame. The WS is organized in New Zealand. From this position, the free leg is released from the floor and the pelvis on the side of the free leg describes a caudal movement in order to then be raised back to the starting position. (See video 13.)
Load normative:
Repetitions: 10, 3 series, break by changing legs
Increase: Increase the number of repetitions by 3 repetitions each time, or increase the series by one series.
Evasive movements:
- The foot of the supporting leg can no longer hold the arch structure of the foot. (See evasion mechanisms, exercise 3 and 4.)
- The supporting leg gives way to a “genu recurvatum”.
The WS leaves NZ.
The difficulty of the exercises, which “appear easy” at first glance, lies in the quality of the exercise.
Intensive care by the therapist in the “practice phase” is therefore essential, as the number of repetitions lead to an “automation process” of the movement patterns.
Feedback from Mr. “AT” after 4 weeks of training:
- “The first days were very painful, but very effective.”
- “I have running results in training, 5 years ago.”
- “Above all, I had less signs of fatigue during and after running.”
- “I feel changes in my right knee; after about 1-2 km, I run completely pain-free.”
- “My stride length has improved.”
- “I run lighter and more relaxed.”
- “The heart rate has dropped by approximately 5-10 beats.”
- Improvements: “With a 10 from approximately 58 minutes to 53-53 minutes; with a 20 from 2:05 to 1: 56-1: 58, and everything at training speed, not full speed.”
This post was translated into English from the original German version available here.
Comments are closed.